

With the number of Americans aged 65 or older projected to reach 83.7 million by 2050, managing care coordination to achieve better outcomes and control costs has become a national priority. Great Plains QIN partners with healthcare systems and communities throughout our region to foster improved coordination to decrease medication errors, unnecessary or repetitive diagnostic tests, unnecessary emergency room visits, and preventable hospital admissions and readmissions.
NEW—A Readmissions Interview Tool was recently developed by Great Plains QIN as a result of care coordination and readmissions conversations with hospital staff. This tool gives the care team and patients/families/caregivers an opportunity to discuss perceptions of their recent hospitalization and post-discharge experience with an added goal of engaging patients as active partners on their care team. The tool is a sneak peek into a Readmissions Toolbox to be released soon that is a compilation of practices and tools to reduce readmissions and improve care coordination.
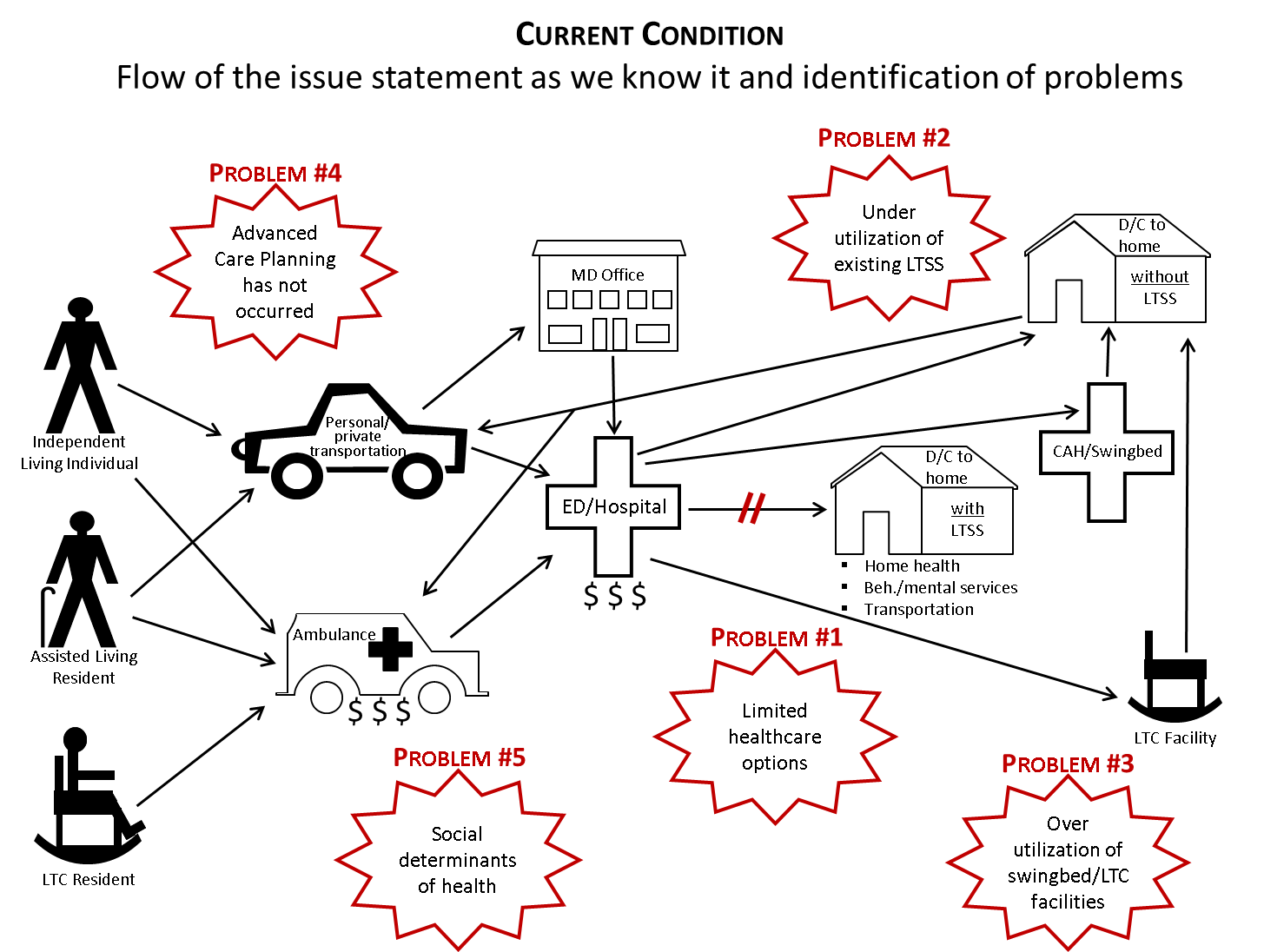
Improved care coordination increases the amount of time people are able to stay in their home, referred to as community tenure. The Great Plains QIN Care Coordination team utilized a quality improvement problem solving process to analyze community tenure data, investigate potential issues affecting community tenure and their root cause, and identify potential solutions. The team identified limited access to or underutilization of Long Term Support Services (LTSS) as a major barrier that leads to potentially decreased community tenure and overutilization of higher levels of care such as skilled nursing facility or swingbed unit as depicted in the “Current Condition” image.
Opportunities for improvement identified by the team include: improving awareness of LTSS, expanding existing models such as community health workers and chronic care management, addressing health literacy and disparities, and increasing the use of advance health directives. Part of the Great Plains QIN response to this was the provision of the following educational Learning and Action Network events.
Learning and Action Network Event Recordings
- Improving Care Coordination by Working with Super-Utilizer Patients
- Super Utilizer Patients Follow-Up Coaching Call
- Improving End-of-Life Care: Eating the Elephant One Bite at A Time
- Chronic Care Management: Medicare and Beyond
- Discharge Processes to Assist in Progression of Care Management
- Teach-Back – Improving Patient Safety and Engagement
- Teach-Back Follow Up Coaching Call
- Bedside Medication Delivery Program (Med-to-Bed) to Reduce Readmissions and Improve Outcomes
Resources
- Great Plains QIN Care Coordination and Medication Safety
- NEW—Skilled Nursing Facility (SNF) Shared Best Practices to Reduce Potentially Preventable Readmissions (PPRs)
- NEW—Patient Readmission Interview Tool
- COMING SOON—Readmissions Toolkit
COMING UP NEXT WEEK ON APRIL 16…
National Care Transitions Awareness Day; hosted by the Centers for Medicare & Medicaid Services (you can still register to attend virtually)
National Healthcare Decisions Day